
SMRUTHI-INDIA involves establishment of a large well-defined cohort of healthy individuals with age ≥ 55 and having risk factors for dementia. This study design of "Cohort Multiple Randomised controlled Trial" combines a cohort study with in-built provisions to do multiple randomised controlled trials. The study design allows the conduct of multiple interventions in the cohort and it reduces the cost of implementation of these studies.
SMRUTHI-INDIA is planned in two phases: Phase 1 will be establishment of the cohort in 4 MRHRUS and development of the multimodal care bundle with a feasibility study. Phase 2 will be evaluation of this multimodal care bundle in a randomised controlled trial.
The first intervention which we plan to implement (in phase 2 of the study) is a locally designed multimodal "care bundle" for prevention of dementia which is culturally tailored and context-specific to Indian population. This will be the first primary prevention strategy ever tested in a high quality Randomised Controlled Trial in India. If proven to be efficacious, this multimodal care bundle can be integrated to the National Health Programmes.









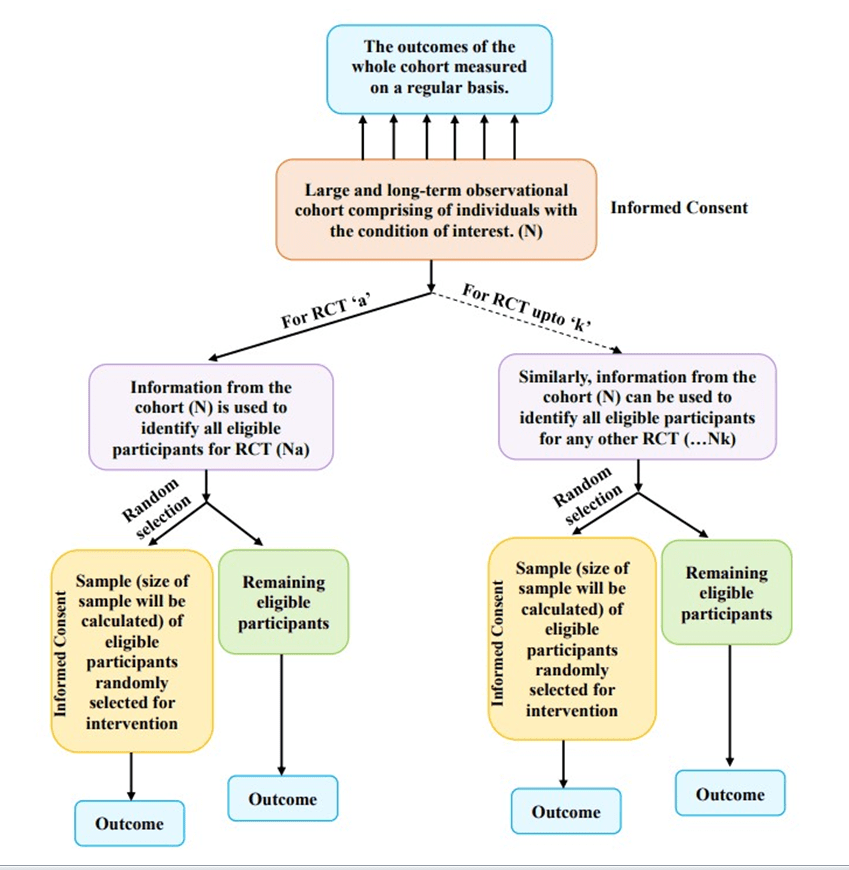
Often missing the mark to meet recruitment targets, higher cost and attrition rate, and possibilities of response bias were some of the major drawbacks of a Randomized Controlled Trial (RCT).3 To tackle some of these weaknesses of RCT, the “Cohort Multiple Randomised Controlled Trial (cmRCT),” also known as the “Trials within Cohorts (TwiCs)” design, was proposed by Clare Relton and colleagues in 2010.
Randomization in the cmRCT design is done before offering the treatment, increasing the possibility that a proportion of those offered treatments may decline. A complier average causal effect (CACE) analysis approach is considered a robust statistical analysis plan as it adjusts for the possibility that considerable numbers of participants may decline the treatment after randomization.



